PHONE
+44-7482-878921
+44-7482-878921
2376-0249
Case Blog - International Journal of Clinical & Medical Images (2017) Volume 4, Issue 1

Author(s): Chin HT, Shai SE and Hu SY*
Boerhaave’s syndrome (spontaneous esophageal perforation) involving a complete and transmural laceration caused by a rapid rise in intraluminal pressure in the distal esophagus is a rare but serious condition with a mortality rate of 20~40%. Late diagnosis or misdiagnosis occurs in more than 50% patients owing to the rarity of classic Mackler’s triad of stretching vomiting, low thoracic pain and subcutaneous emphysema. Herein, we reported a case of Boerhaave’s syndrome in a 71-year-old man presenting chest pain, dyspnea on exertion and orthopnea for 1 day after stretching vomiting. Chest X-ray and computed tomographic scan showed subcutaneous emphysema of neck, pneumomediastinum and lobulated pleural effusion suggestive of esophageal perforation. Immediate left thoracotomy with primary repair for a 2 cm esophageal perforation over left anterolateral side above the esophagogastric junction was performed. The culture of pleural effusion yielded Klebsiella pneumoniae, Citrobacter koseri and Pseudomonas fluorecens. He was discharged on the twenty-sixth day.
Boerhaave’s syndrome, a spontaneous esophageal perforation involving a complete and transmural laceration caused by a rapid rise in intraluminal pressure in the distal esophagus, is a rare but serious condition with a mortality rate of 20~40%. Late diagnosis or misdiagnosis occurs in more than 50% of patients because of the rarity and the absence of the classic Mackler’s triad of stretching vomiting, low thoracic pain and subcutaneous emphysema. The perforation is usually in the lower third and left lateral position of the esophagus due to an anatomic weakness. Diagnostic tools included chest X-ray, computed tomographic (CT) scan, esophagogram, and esophagoscope. Factors that influence the prognosis are the time interval between onset of injury and primary repair, and the underlying physical status.
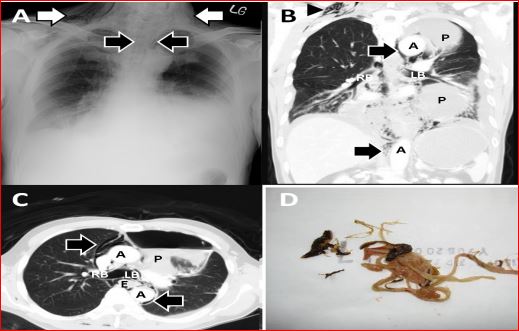
A 71-year-old health Taiwanese man presented to our emergency department with low thoracic pain, dyspnea on exertion and orthopnea for one day after stretching vomiting. On arrival, the vital signs were a respiratory rate of 22 breaths per minute, a pulse rate of 108 beats per minute, a blood pressure of 100/44 mmHg, and a body temperature of 35.5ºC. Physical examination revealed mild cardiopulmonary distress, decreased breathing sound over left lower lung and basal rales over bilateral lower lung fields, rapid regular heart beats and soft abdomen with normoactive bowel sound. Laboratory evaluation showed white blood cell counts of 4.8 × 103 /mm3 with 87.4% of neutrophils, hemoglobin 13.6 of g/dl, blood urea nitrogen of 39 mg/dl, creatinine of 2.4 mg/dl, glucose of 233 mg/dl, C-reactive protein 8.7 of mg/dl and others are unremarkable. Arterial blood gas revealed pH of 7.287, PaCO2 of 24.3 mmHg, PaO2 of 110 mmHg, BEB of-12.4 and HCO3 - of 11.7 mmol/l. Chest X-ray (Figure 1A) showed subcutaneous emphysema over right neck, pneumomediastinum and air-fluid level in left lung field. Axial and coronal views (Figure 1B and 1C) of chest CT scan demonstrated subcutaneous emphysema over bilateral neck, pneumomediastinum with air surrounding aorta, esophagus, and bronchus, and lobulated pleural effusion with air-fluid level suggestive of spontaneous esophageal perforation (Boerhaave’s syndrome) with the classic Mackler’s triad of stretching vomiting, low thoracic pain and subcutaneous emphysema. Immediate left thoracotomy with primary repair for a 2 cm esophageal perforation with well-defined mucosal margin over the left anterolateral side above the esophagogastric junction, decortication, pneumolysis with gastrostomy and jejunostomy were completed. 300 ml of dirty fluid containing mushroom and food material (Figure 1D) in left anterosuperior pleural space with diffuse and sticky pleural adhesion were noted on operative findings. The culture of pleural effusion yielded Klebsiella pneumoniae, Citrobacter koseri and Pseudomonas fluorecens. Esophagography showed a small crater over the left lateral wall without significant leakage on the 12th day. He was discharged on the 26th day.
Boerhaave’s syndrome, a spontaneous esophageal perforation involving a complete and transmural laceration caused by a rapid rise in intraluminal pressure in the distal esophagus, is a rare but serious condition with a mortality rate of 20~40% [1-5]. There are uncommon presentations with the classic Mackler’s triad of stretching vomiting, low thoracic pain and subcutaneous emphysema, hence causing delayed diagnosis [2-5]. Late diagnosis or misdiagnosis occurs in more than 50% of patients because of the rarity and the absence of the classic symptoms, so Boerhaave’s syndrome often presents a diagnostic challenge [1,2]. The perforation is usually (around 90% of cases) in the lower third and left lateral position of the esophagus due to an anatomic weakness allowing gastric contents direct access to the mediastinum and pleural cavity, leading to severe mediastinitis and empyema [1,3]. Diagnostic tools included chest X-ray, CT, esophagography, and esophagoscope [1-5]. Factors that influence the prognosis are the time interval between onset of injury and primary repair, and the underlying physical status. The 24 h delay after perforation is often considered as the main factor influencing mortality [1-5]. There are four aims in management strategy, including (1) Considered direct repair if possible. Functional or surgical isolation of esophagus from stomach was suggested if not possible; (2) Adequate drainage; (3) Appropriate antibiotics; (4) Adequate feeding [2].
 Awards Nomination
Awards Nomination