PHONE
+44-7482-878921
+44-7482-878921
2376-0249
Case Blog - International Journal of Clinical & Medical Images (2016) Volume 3, Issue 6

Author(s): Keisuke Nakabayashi, Toshiaki Suzuki, Hisayuki Okada and Toshiaki Oka
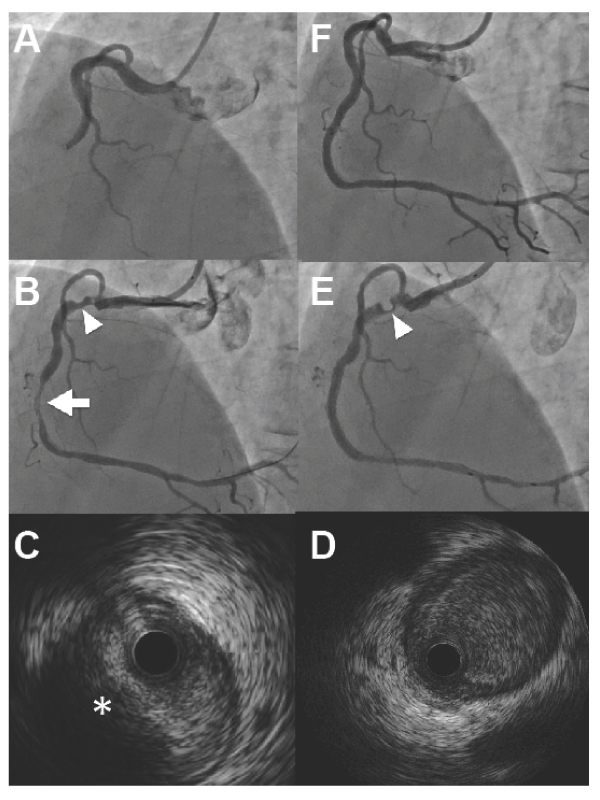
Clinical Presentation: A 64-year-old man was diagnosed with recent myocardial infarction by previous chest pain and ischemic electrocardiography changing. He underwent coronary angiography 1 week after the first symptom, which revealed total occlusion of the middle right coronary artery (RCA) with moderate tortuosity (Figure 1A). After crossing the soft guidewire and pre-dilation of the culprit lesion, the eccentric stenosis occurred at the proximal RCA (Figure 1B). The first intravascular ultrasonogram (IVUS) showed an oval-shaped narrowing and attenuating findings like vulnerable plaque (Figure 1C). We continued the percutaneous coronary intervention to distal RCA with the filter guidewire (Parachute, Tri-Med, Osaka, Japan). Everolimus-eluting stent was put in the culprit lesion. The second IVUS showed no stenosis after distal stenting (Figure 1D), although angiographic stenosis got worse (Figure 1E). We could confidentially retrieve the wire, which resolved the pseudostenosis completely (Figure 1F), as expected. A coronary accordion phenomenon caused by mechanical alteration is not uncommon. IVUS is helpful for ruling out a dissection, spasm, or thrombus formation, but it does not have specific findings [1]. The present case demonstrates different IVUS findings before and after distal stenting. The IVUS images at the accordion phenomenon site sometimes differ from angiographic findings. Coronary flow might influence this discrepancy. To avoid unnecessary stenting, repeated IVUS investigation is recommended if coronary flow changes.
 Awards Nomination
Awards Nomination