PHONE
+44-7482-878921
+44-7482-878921
2376-0249
Clinical Image - International Journal of Clinical & Medical Images (2021) Volume 8, Issue 11

Author(s): Ben Jmaa Hela*, Mhiri Fatma, Gueldich Majdi, Fendri Sami, Rejab Haitham, Dammak Aiman and Frikha Imed
Abstract
Abdominal aortic aneurysms are defined as focal dilatations of the abdominal aorta that are 50% greater than the proximal normal segment. The complications of these aneurysms include rupture, infection, aorto-enteric and aorto-caval fistulas, embolic occlusion of branch vessel, and compression of adjacent structures. Aorto-enteric fistulas can be primary, caused by atherosclerotic aortic aneurysm or secondary related to from aortic reconstructive surgery. We report a rare case of a saccular abdominal aortic aneurysm ruptured into the first jejunal loop treated surgically.
Keywords: Aortic aneurysm; Complications; Aorto enteric fistula; Surgery
Clinical Image
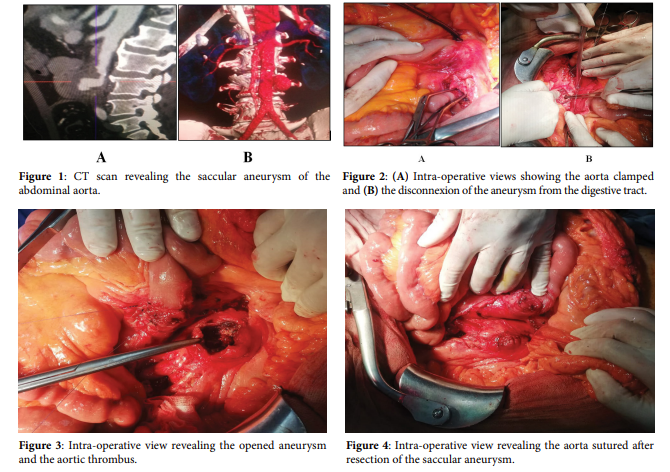
A 77-year-old man, diabetic since 2009, operated for gastric ulcer on 2014, who had a non-operated renal lithiasis, was admitted to the department of visceral surgery for melena since 2 days. On arrival in our hospital, vital signs were, the blood pressure was 120/60 mm Hg, the heart rate was 106 beats per minute, and the body temperature of 36.5°C. Physical examination revealed also an operative scar over middle abdomen. There were no signs of portal hypertension. Melenas were objectified in the rectal examination. His hemoglobin rate was 10.7 g/dl, hematocrit was 30.2%, and platelet rate was 205000/mm³. He had a correct level of renal and liver function. The patient had a fibroscopy which showed a hiatal hernia complicated with fragile peptic esophagitis stage A of Los Angelos, a gastritis and congestive bulbitis. A colonoscopy was made objectified a non-specific ulcerated sigmoiditis, a colonic polyp, internal hemorrhoids with a hard and with irregular wall, and perianal loss of substance, the biopsy concluded that the focal colitis was of infectious origin most likely. He stayed hemodynamically stable. Control haemoglobin rate performed at fifth day of hospitalization was equal to 9.9 g/dl. The patient was put out of the hospital with antibiotics and anemia treatment. After 10 days, he was readmitted to our department because of a second episode of melena. He had a blood pressure of 110/60 mmHg, a heart rate of 78 beats per minute. His haemoglobin rate was 8.1 g/dl, haematocrit was 25%. We controlled haemoglobin rate after 12 hours. It was equal to 7.3 g/dl. After 24 hours, it was equal to 6.6 g/dl. An emergency CT scan was performed. It showed an aneurysm of the aorta fistulated in the first jejunal loop (Figure 1). The patient underwent emergent surgery under medial laparotomy. On macroscopic examination, we found an adhesion between the first jejunum and sacciform aneurysm of the abdominal aorta. We controlled and dissected the supra aneurysmal aorta and two primary iliac arteries. After general heparinization, we clamped the aorta and disconnected it of the digestive tract bag (Figure 2). We opened the aneurysm, evacuated the wall thrombus, and washed of the aortic lumen with heparinized serum (Figure 3). Good reflow from the iliac arteries and good flow from the aorta was found. Then, the aortic wall was sutured by two round trip hemi-projects (Figure 4). After venting and declamping, the presence of good pulses in the primary iliac arteries was checked. We closed the aneurysmal horn on a Redon drain number 16. The jejunal cove was sutured by separate stitches with 3/0 absorbable sutures, and drained next to it by probe Delbert blade and Salem probe. The initial postoperative outcomes were favourable, he had a stable hemodynamic state, no fever, abdominal examination revealed no abnormalities, he had a correct diuresis, and no bleeding in the drains. Haemoglobin at first post-operative day was 9.8 g/dl. The patient received on unfractionated heparin in the immediate postoperative period with a dose of 80 mg with the electric syringe push. This treatment was stopped at the third post-operative day because of a bleeding in the Redon. He received a preventive dose of low-molecular-weight heparins (LMWH) with and platelet aggregation inhibitor dosed of 100 mg twice a day. The removal of the nasogastric tube was performed at the fifth day. At the tenth day, he presented a digestive fistula marked by the release of digestive fluid at the drainage putted opposite the duodenal suture. He received antibiotics with local care. Then, the patient presented a respiratory distress. He was polypneic. His oxygen saturation was 75%. The patient was transferred to the intensive care unit and received mechanical ventilation. Two days later, he died from respiratory distress, probably related to basal pneumonia.
Comments
Abdominal Aortic Aneurysms (AAA) are defined as focal dilatations of the abdominal aorta that are 50% greater than the proximal normal segment. The most common location includes infrarenal with extension into iliac arteries. Imaging is essential for the detection of AAA, monitoring of rate of growth, pre-operative planning and post-operative follow-up.
Computed tomography scan has become an integral part of the evaluation of abdominal aortic aneurysms and has virtually replaced conventional angiography for the evaluation of these aneurysms [1]. MR angiography can provide the same information as CT scan [2]. These investigations show saccular shape in mycotic aneurysms as opposed to fusiform shape in atherosclerotic aneurysms [3]. The complications of these aneurysms include rupture, infection, aorto-enteric and aorto-caval fistulas, embolic occlusion of branch vessel, and compression of adjacent structures. Aorto-enteric fistulas can be primary, caused by atherosclerotic aortic aneurysm or secondary related to from aortic reconstructive surgery. The most commonly involved part of the gut third and the fourth portions the duodenum. Symptoms usually include abdominal pain, hematemesis, and melena. Treatment of these fistulas is emergent surgery of resection of the aneurysm and enteric reconstruction.
Declaration of Interests
Both authors have no conflicts of interest to disclose.
References
Haberler
Haberler
Haberler
Haberler
Haberler
Haberler
Haberler
Haberler
Haberler
Haberler
Haberler
Haberler
Haberler
Haberler
Haberler
Haberler
Haberler
Haberler
Haberler
Haberler
Haberler
Haberler
Haberler
Haberler
Haberler
Haberler
Haberler
Haberler
Haberler
Haberler
Haberler
Haberler
Haberler
Haberler
Haberler
Haberler
Haberler
Haberler
Haberler
Haberler
Haberler
Haberler
Haberler
Haberler
Haberler
Haberler
Haberler
Haberler
Haberler
Haberler
 Awards Nomination
Awards Nomination