PHONE
+44-7482-878921
+44-7482-878921
2376-0249
Clinical-Medical Image - International Journal of Clinical & Medical Images (2023) Volume 10, Issue 3

Author(s): Amine Cherraqi1*, Zakaria Abide2, Hajar Andour2, Sahar Merbouh2, Siham El Haddad2, Nazik Allali2 and Latifa Chat2
1Department of Radiology, Mohammed Vth Military Hospital, Rabat, Morocco
2Department of Radiology, Children Hospital of Rabat, Ibn Sina University Hospital, Faculty of Medicine and Pharmacy of Rabat, Morocco
Received: 11 March 2023, Manuscript No. ijcmi-23-91366; Editor assigned: 13 March 2023, Pre QC No. P-91366; Reviewed: 27 March 2023, QC No. Q-91366; Revised: 31 March 2023, Manuscript No. R-91366; Published: 07 April 2023, DOI:10.4172/2376-0249.1000882
Citation: Cherraqi A, Abide Z, Andour H, Merbouh S and Haddad SE, et al. (2023) Essential Bone Cyst: Fallen Fragment Sign and Trap Door Sign. Int J Clin Med Imaging 10:882.
Copyright: © 2023 Cherraqi A, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
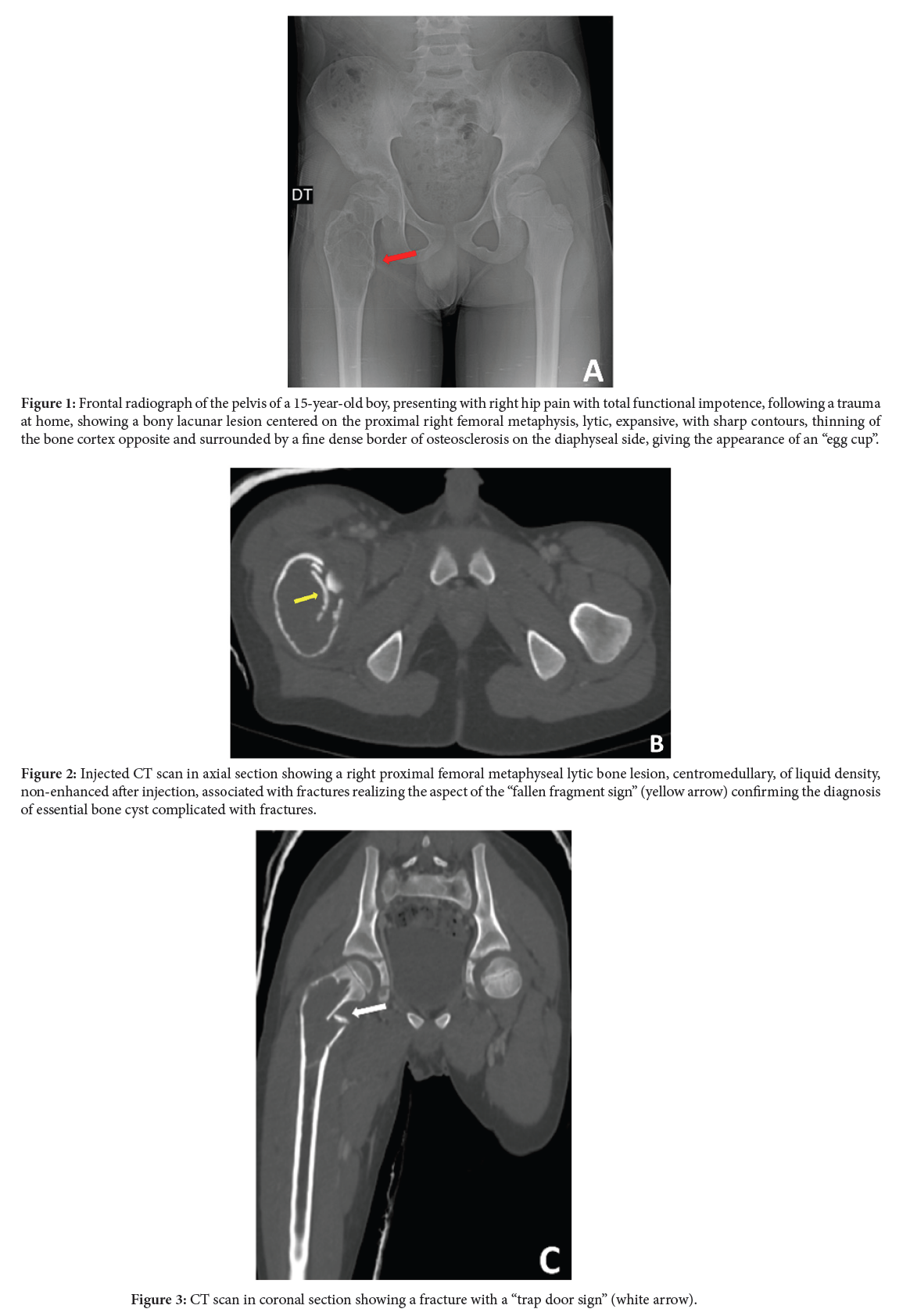
The essential or solitary or unicameral bone cyst is a cystic bone dystrophy of unknown origin producing a pseudo-tumor lesion, in the form of a uni or plurilocular metaphyseal bone cavity weakening the bone and containing a clear, lemon-yellow, but sometimes hemorrhagic fluid [1]. It affects mostly children between 5 and 15 years of age, with a predominance of males, is most often discovered by chance [2], is often unique and is generally located on the upper metaphysis of the long bones (humerus 50%, femur 25%, tibia) [1,2]. On standard radiography, the typical KOE appears as an ovoid lacuna of geographic osteolysis, without a septum, centered in the metaphyseal region in contact with the conjugation cartilage, with a major axis parallel to the bearing bone, with clear, well-limited contours, with peripheral sclerosis, more accentuated on the diaphyseal side, creating the “egg cup” appearance (Figure 1). The cortices are thinned but respected. It may contain fine internal septa [1]. The CT scan reveals a thin-walled, often pseudoseptate, osteolytic lesion with fluid density. Its main interest is to evaluate the thickness of the cyst walls, the potential fracture risk and the extension of the lesion into a complex region, such as the spine or pelvis [1]. Fracture is the most frequent mode of revelation. Two radiographic aspects can be found: -the pathognomonic “fallen fragment sign”, corresponding to the presence of cortical fragments that settle at the bottom of the cyst and that change position with the patient’s mobility [1,2] (Figure 2) and the “trap door sign” with the fractured bone fragment remaining attached to the periosteum (Figure 3) [1]. MRI confirms the cystic nature of the lesion. The typical KOE appears as a single lacuna, without septa with fluid content in hyposignal T1 hypersignal T2. After injection of gadolinium, the periphery of the cyst and any septa may be enhanced. A liquid level is rarely found. A fractured KOE may be the site of fluid levels with intracystic hemorrhage and sedimentation of old blood and may show pseudonodular enhancement [1,2].
Essential bone cyst; Fallen fragment sign; Trap door sign; Imaging
The authors declare that they have no conflict of interest in relation to this article.
[1] Mascard E. (2014) Kystes osseux: Kyste osseux essentiel et kyste osseux anévrysmal. Conférences d'enseignement: 171.
Google Scholar, Crossref, Indexed at
[2] Docquier PL and Schubert T. (2015). Solitary bone cyst: 31-490-A-10.
 Awards Nomination
Awards Nomination