PHONE
+44-7482-878921
+44-7482-878921
2376-0249
Clinical-Medical Image - International Journal of Clinical & Medical Images (2023) Volume 10, Issue 6

Author(s): Akash Anand Dobhada*, Shivam Bajpai and Manoj Kumar Sahu
Department of Gastroenterology, Apollo Hospital, Bhubaneswar 751005, India
*Corresponding Author:
Akash Anand Dobhada
Department of Gastroenterology
Apollo Hospital, Bhubaneswar 751005, India
Tel: +91 9090829127
E-mail: akashdobhada007@gmail.com
Received: 24 May 2023, Manuscript No. ijcmi-23-99795; Editor assigned: 25 May 2023, Pre QC No. P-99795; Reviewed: 08 June 2023, QC No. Q-99795; Revised: 13 June 2023, Manuscript No. R-99795; Published: 20 June 2023, DOI:10.4172/2376-0249.1000900
Citation: Dobhada AA, Bajpai S and Sahu MK. (2023) Jejuno-Gastric Intussusception with Gangrene of Jejunal Segment-A Case Report of Rare Life-Threatening Complication of Gastro- Jejunostomy. Int J Clin Med Imaging 10: 900.
Copyright: © 2023 Dobhada AA, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Jejunogastric intussusception is rare complication. We present a case of young patient presented with pain abdomen and hematemesis. On evaluation found to have jejuno-gastric intussusception with gangrene of jejunal segment. Urgent laparotomy was done. Gangrenous segment was resected. Early detection and early surgical intervention is necessary for prevention complication.
Jejunogastric intussusception is rare complication of gastric surgeries and the incidence is around 0.1% [1]. This type of intussusception can occur in different types of gastric surgeries for example gastrojejunostomy, Billroth II and Roux en Y reconstruction [2]. According to literature, this type of intussusception can occur after few days to up to 25 years post operation [3]. We encountered a young patient who presented with pain abdomen, hematemesis and shock. Patient required urgent surgical intervention.
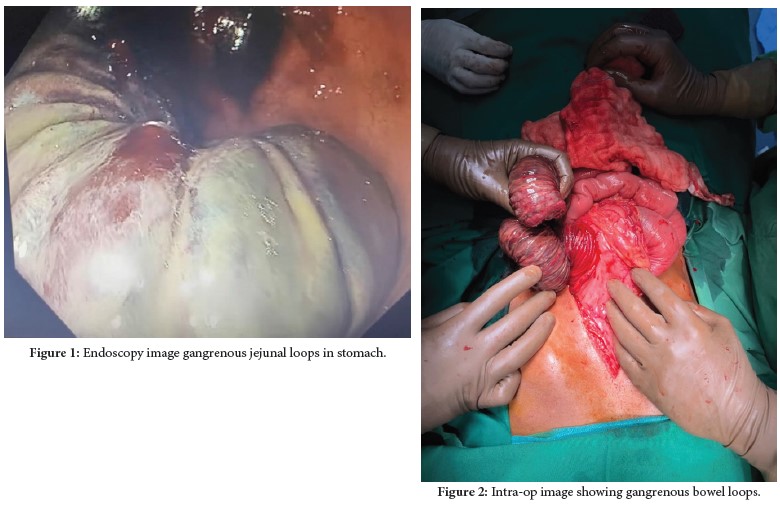
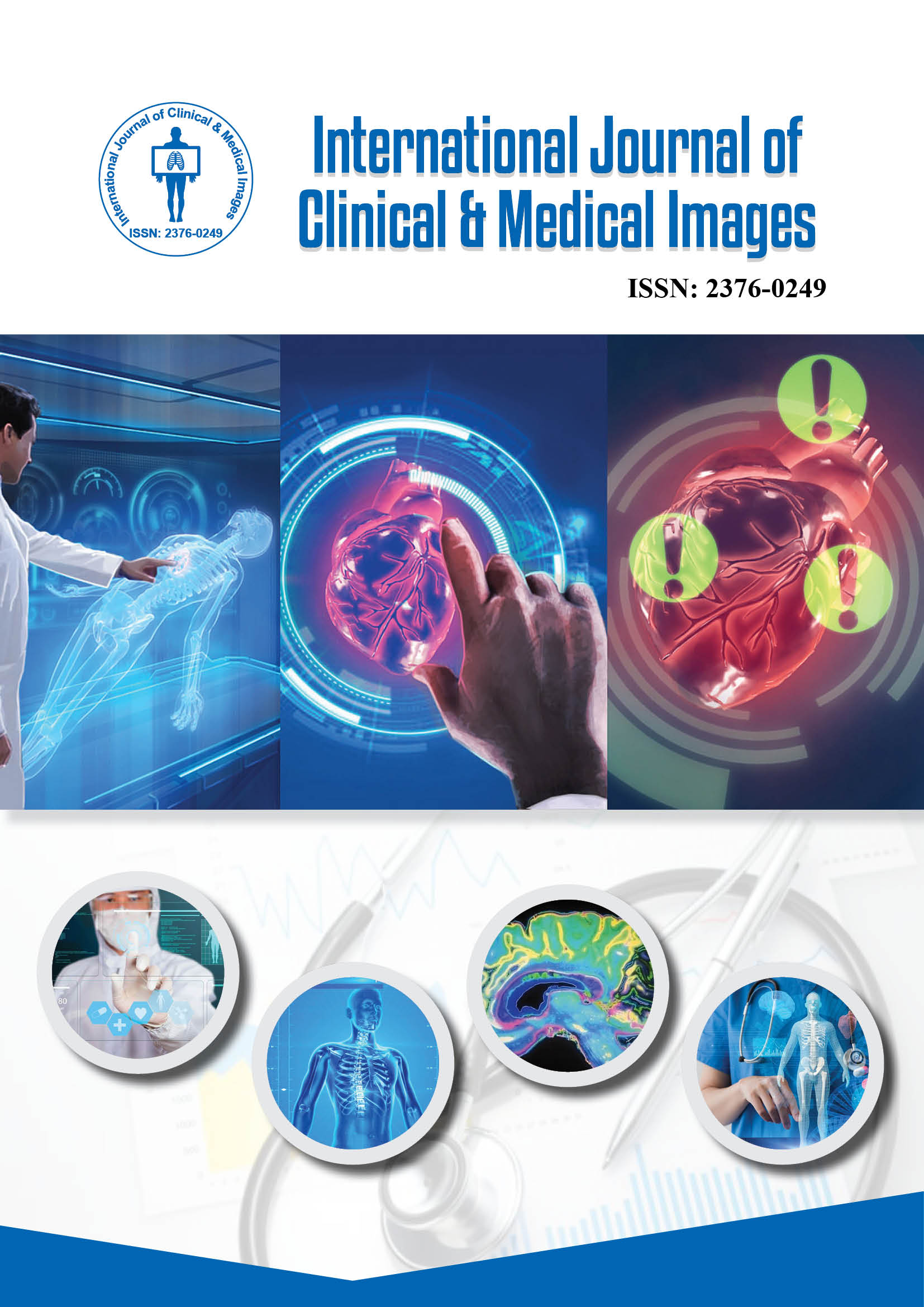
38 years old male presented to emergency department with chief complaints of multiple episodes of hematemesis, pain in abdomen for 3 days. Pain was diffuse, more in epigastric region, continuous and not associated with aggravating or relieving factors. Patient had history of Gastrojejunostomy 4 years back for peptic ulcer disease. Patient was on presentation to emergency department was in shock with tachycardia and low blood pressure. Patient had midline incision scar. On palpation, abdomen was mild tender in epigastric region, bowel sound was sluggish. Patient was unstable; hence patient was admitted in ICU and started resuscitation with IV fluids, PRC transfusion. Patient was taken for endoscopy once he was stable. Endoscopy showed jejunal loops prolapsed retrogradely into stomach with twisting of loops; bowel mass appears greyish- black s/o bowel gangrene. Small quantity of blood was noted in gastric lumen; no fresh bleeding noted. Urgent surgical call was given and patient was taken to OT for emergency exploratory laparotomy. Operative findings: Midline incision was given, scar tissue excised, anterior gastrostomy was done. Gangrenous jejunal loops identified; Gastro-jejunostomy was dismantled; gangrenous jejunal loops resected. Pyloric dilation done with finger; jejuno-jejunal end to end anastomosis was done; 2 drains were placed in abdomen and incision closed in layers.
Histopathology report
• Gross specimen description: Small intestinal segment 19 cm long. On cut open the intussusceptum 9 cm long. The intusscipien deeply congested and gangrenous. Other cut open segment of intestine mucosa appears viable.
• Microscopic description: Section from intusscipiens and intsssceptum region showed segmental necrotic mucosa with underlying submucosa showing dilated and congested blood vessels. Adjacent mucosa showed denudation of surface epithelium, dense inflammation in lamina propria, underlying submucosa oedematous, congested with areas of fibrin deposits in congested serosa. Surgical cut margins showed focal surface epithelial ulceration, denudation and congested blood vessels and acute inflammatory cells in submucosa and serosa.
Post operatively patient was kept in ICU for 3 days for observation. Patient was given broad spectrum iv antibiotics, multiple Packed red cell transfusion. Gradually patient showed signs of improvement. Orally diet was started which he tolerated well. Drains were removed on post OP Day 5. Sutures removed on post OP Day 10. Patient was discharged in clinical stable state.
Jejunogastric intussusception is rare complication in which the afferent loop or efferent loop of jejunum or both loops invaginated into stomach from gastrojejunostomy stoma site. In 1940 Shackman classified Jejunogastic intussusception into three types depending upon which loop invaginated. Type I – afferent loop intussuscepted into stomach, type II- Efferent loop intussuscepted into stomach and Type III – both afferent and efferent loops intussuscepted into stomach. In our case, both loops were intussuscepted hence it was Type III [4]. The exact cause of these type of intussusception in not known. Two major theories for cause of intussusception are functional and mechanical. Functional theory is widely accepted. Few postulated causes are long afferent loop, jejunal spasm, increased mobility of efferent loop and adhesions. Jejono-gastric intussusception are reported in cases post operatively immediately and, in few cases, up to 55 years post procedure [5-7]. The presentation of intussusception varies. In acute cases there is pain in abdomen, intestinal obstruction, palpable mass per abdomen and hematemesis. Some cases may present with chronic intussusception. The symptoms of chronic intussusception are epigastric fullness, intermittent vomiting [7]. For diagnosis of jejuno-gastric intussusception, we need high index of suspicion. Early diagnosis is the key to prevent serious complications like gangrene. Delay in detection can cause increased mortality up to 50% if delay in diagnosis by 48 hours. The imaging like plain x ray abdomen and USG abdomen can help in diagnosis but contrast CT scan can detect intussusception more easily and it confirms the diagnosis. UGI endoscopy helps in detection of intussusception as well as can show mucosal viability but there are limitations due to limited view in endoscopy. There are few reports of endoscopic reduction of intussusception but, recurrence rate and risk of perforation is high [2]. Surgery is treatment of choice. Emergency surgery necessary in most cases to prevent serious complication and clinical deterioration. Usually, simple reduction or resection and refashioning of gastroenterostomy done. Fixation of reduced jejunal loop to adjacent tissue may be considered for preventing recurrence [7].
Jejuno gastric intussusception is rare but life-threatening complication of past gastric surgeries. High index of suspicion in necessary. Early surgical intervention prevents life threatening complications.
Jejuno-gastric intussusception; Upper GI bleeding; Gangrene
None of the authors has any conflicts of interests to disclose.
[1] Waits JO, Beart RW and Charboneau JW. (1980). Jejunogastric intussusception. Arch Surg 115: 1449-1452.
Google Scholar, Crossref, Indexed at
[2] Lee SH, Kwon IG, Ryu SW and Sohn SS. (2014). Jejunogastric intussusception: A rare complication of gastric cancer surgery. Int J Clin Exp Med 7: 4498.
[3] Conklin EF and Markowitz AM. (1965). Intussusception, a complication of gastric surgery. Surgery 57: 480-488.
Google Scholar, Crossref, Indexed at
[4] Ralph S. (1940). Jejunogastric intussusception. Br J Surg 27: 475–480.
[5] Robertson DS and Weder CH. (1968). Acute jejunogastric intussusception. Can J Surg 11: 210-214.
[6] Bundrick TJ and Turner MA. (1981). Retrograde jejunogastric intussusception. Niger J Surg 6: 21-24.
Google Scholar, Crossref, Indexed at
[7] Tokue H, Tsushima Y, Arai Y and Endo K. (2009). Jejunogastric intussusception: Life-threatening complication occuring 55 years after gastrojejunostomy. Intern Med 48: 1657-1660.
 Awards Nomination
Awards Nomination