PHONE
+44-7482-878921
+44-7482-878921
2376-0249
Clinical-Medical Image - International Journal of Clinical & Medical Images (2022) Volume 9, Issue 2

Author(s): Maryaa Koeter
Received: 03 February, 2022, Manuscript No. M.No: ijcmi-22-55466; Editor assigned: 04 February, 2022, PreQC No. P-55466; Reviewed: 18 February, 2022, QC No. Q-55466; Revised: 23 February, 2022, Manuscript No. R-55466; Published: 28 February, 2022, DOI: 10.4172/2376-0249.1000812
Clinical-Medical Image
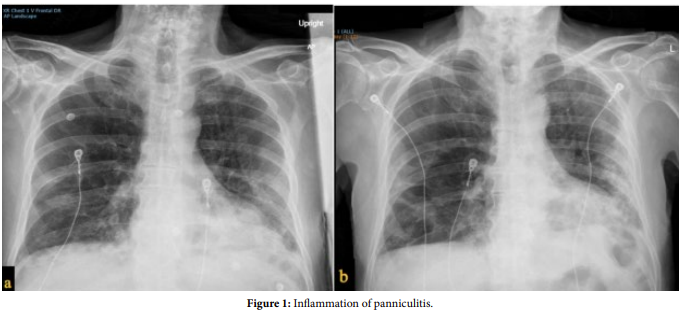
A 65-year-old man presented with syncope and dyspnoea secondary to COVID-19 infection. He developed acute respiratory distress syndrome with subsequent bilateral pulmonary emboli despite intravenous heparin therapy on admission. Chest computed tomography revealed large bilateral acute pulmonary emboli with right ventricular strain. Echocardiogram showed an estimated ejection fraction of 55% with dilated inferior vena cava, right atrium, and right ventricle. The patient’s oxygen requirements continued to increase necessitating endotracheal intubation and mechanical ventilation. On ventilation he required a tidal volume of 340, respiratory rate of 28, PEEP of 14, and FiO2 of 100%. The patient was themodynamically unstable with increasing oxygen demand in the setting of massive pulmonary embolism with right ventricular strain, so mechanical thrombectomy was performed. Right heart catheterization showed peak pulmonary artery pressure of 45mmHg with mean of 30 mmHg. Significant amount of clot burden was removed from the right upper and middle lobes as well as the left middle lobe using INARI 24 Flow Triever. Post-injection revealed good perfusion in all the lung lobes. Following clot removal the mean pulmonary artery pressure dropped by >10 mmHg and the FiO2 reduced to 70%. Mechanical thrombectomy has been shown to reduce pulmonary artery pressure by a mean of 8 mmHg. This method has a lower risk of bleeding at 6.7%, and a 30-day mortality benefit of 8.0% [1]. This vignette presents images of a mechanical thrombectomy as the first line treatment modality for pulmonary embolism in the setting of acute respiratory failure with hemodynamic instability due to SARS-CoV-2 (Figures 1-5).
Keywords: Pulmonary embolism: Mechanical thrombectomy; COVID-19
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Reference
[1] Patel NJ, Atti V, Basir MB, and Aggarwal V (2019) Catheter based therapies in massive pulmonary embolism. Int J Cardiol 287: 116-117.
 Awards Nomination
Awards Nomination