PHONE
+44-7482-878921
+44-7482-878921
2376-0249
Clinical Image - International Journal of Clinical & Medical Images (2017) Volume 4, Issue 6

Author(s): Gashi AM
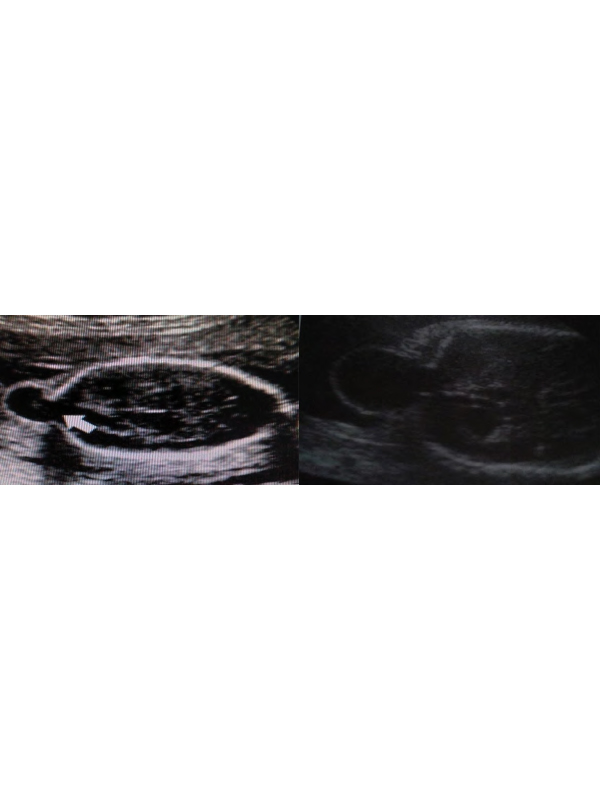
Clinical Image: A 37-year-old woman presented in the Obstetrics and Gynecology Clinic, for the evaluation of pregnancy, which was in the 20th week of gestation. The patient had received a diagnosis for congenital fetal anomalies, by her doctor, who had followed her pregnancy. The patient had no earlier personal history of congenital fetal anomalies, and she had no family history of congenital anomalies. Ultrasound examination showed a skull defect, localized in the occipital region that was a cystic formation or cephalocele. This anomaly was shown with a transthalamic view. The condition is characterized by protrusion of intracranial structures through a cranial bone defect. The herniated anatomic structures can consist of meninges only (meningocele) or meninges plus cerebral tissue (encephalomeningocele). The most common location of cephaloceles is occipital region, but it can also be on frontal region, parietal, occipital, frontoethmoidal, etc. There is an incidence around 1 in 5000 to 1 in 100 000 at birth, but decreasing due to prenatal diagnosis. It is generally thought that cephalocele is caused by a lack of fusion of the neural tube in its specific closing sites. For a correct evaluation of the encephalic structures, apart ultrasound examination in different plans often needed an MRI-scan. During differential diagnosis, the most important lesions to differentiate from occipital meningocele are cystic hygroma, teratoma, and hemangioma. When we have a cephalocele be detected in a fetus, a thorough search for possibly associated structural anomalies has to be carried out (Figure 1). Delivery by cesarean section is advisable to avoid trauma and infection (through the delivery canal) of the exposed brain tissue. Small cephaloceles can be corrected surgically. Very large lesions have an unfavorable prognosis hence there is no benefit from treatment. The postnatal mortality rate varies from 30% to 50%, depending on the dimensions and the location of the lesion, in the presence of cerebral tissue in the herniated sack, etc.
 Awards Nomination
Awards Nomination