PHONE
+44-7482-878921
+44-7482-878921
2376-0249
Clinical-Medical Image - International Journal of Clinical & Medical Images (2024) Volume 11, Issue 1

Author(s): Sanae Jellal*, Amine Neggar, Sara Ez-Zaky, Jihane El Houssni, Ouadie El Menaoui and Abdelaziz Hoummadi
Department of Radiology, Mohammed Vth Military Hospital, Rabat, Morocco
*Corresponding Author:
Sanae Jellal
Department of Radiology
Mohammed Vth Military Hospital
Rabat, Morocco
Tel: 00212604460201
E-mail: sanaejellal@gmail.com
Received: 13 December 2023, Manuscript No. ijcmi-24-122626; Editor assigned: 15 December 2023, Pre QC No. P-122626; Reviewed: 29 December 2023, QC No. Q-122626; Revised: 04 January 2024, Manuscript No. R-122626; Published: 12 January 2024, DOI:10.4172/2376-0249.1000932
Citation: Jellal S, Neggar A, Ez-Zaky S, Houssni JEI and Menaoui OEI, et al. (2024) Perirenal Urinoma on Rupture of the Fornix Secondary to a Bladder Tumour. Int J Clin Med Imaging 11: 932.
Copyright: © 2024 Jellal S, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
The occurrence of urine extravasation due to a ruptured renal fornix is an uncommon complication, primarily attributed to obstruction resulting from distal ureteric stones. Here, we present a case involving the rupture of the fornix associated with a bladder tumor.
Forniceal rupture; Urinoma; Ureteric obstruction; Bladder tumor
The rupture of the fornix is an infrequent occurrence that can manifest at any age, typically arising as a result of calculi. Neoplasms rarely contribute to the formation of urinomas. This case report details a fornix rupture secondary to a bladder tumor.
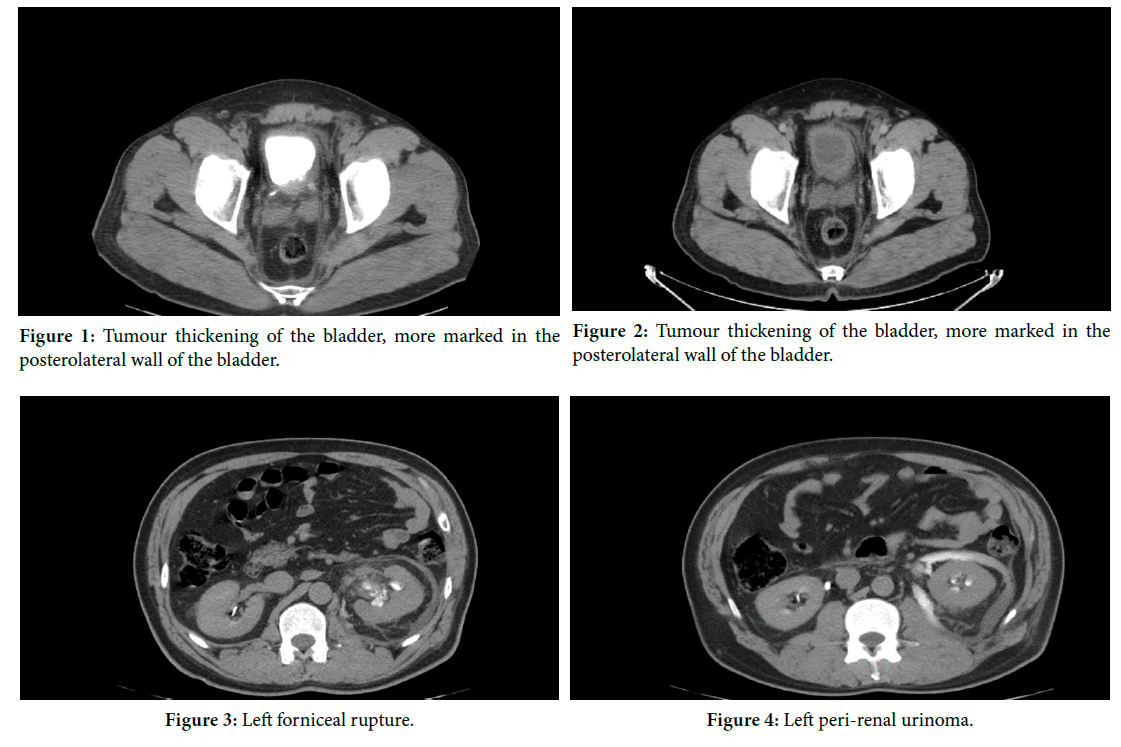
An 55-year-old man, a chronic smoker, has been experiencing left low back pain and intermittent hematuria for the past 6 months, without any additional associated symptoms. These symptoms have developed in a context of apyrexia, and the patient, maintaining overall well- being, decided to seek consultation at the urological emergency department. Upon clinical examination, the patient was conscious, with stable hemodynamics and respiratory function, and showed no signs of fever. The conjunctiva appeared normocolored, and there was sensitivity noted in the left lumbar fossa. A digital rectal examination revealed a prostate estimated at 29 grams, with the base of the bladder slightly infiltrated on the left side but remaining mobile. The rest of the examination did not yield any specific findings. In terms of laboratory assessments, the hemoglobin level was 10 g/dl, indicating a slightly impaired renal function (Creatinine: 13 mg/l, Urea: 0.4 g/l), a CRP level of 50 mg/l, and a clean urine culture. Abdominal ultrasonography identified moderate left uretero-hydronephrosis with anechoic peri-renal effusion, along with a heterogeneous lesion observed on the left posterolateral wall of the bladder.
We supplemented the evaluation with a URO-CT, revealing indications of a tumor on the left posterolateral wall of the bladder (Fig. 1), leading to ureterohydronephrosis and a urinoma, likely due to the rupture of the fornix (Fig. 2).
The rupture of the fornix is a mechanism for releasing the the hyperpressure exerted on the renal parenchyma, the renal sinus and the fascia of Gerota. Rupture during acute is of mechanical origin. In chronic pathologies, it is the progressive appearance of hydronephrosis linked to the reflux of associated with the reflux of urine into the pyelocecal tract which has an irritant effect on the urothelial tissue and responsible for an inflammatory reaction and fibrosis fibrosis [1,2]. Retroperitoneal fibrosis associated with mechanical compression of the lower ureter by the ovarian mass explains ureteral dilatation, the ultimate stage of which is rupture of the cavities. is rupture of the cavities.
The clinical signs are not specific, and renal colic is the most frequent, the diagnosis is most often delayed [3]. In previous studies, fever and leukocytosis are most often absent, as in our case [4].
In addition to treating the cause, the treatment is based on antibiotic therapy to prevent infection of the urinoma, [5] and to insert a ureteral catheter percutaneous nephrostomy in the most severe cases. The literature acknowledges the performance of the double J catheter as first-line treatment in the treatment of fornix ruptures. By allowing emptying of the urinary tract, there is a reduction in pressure in the pyelo-caliceal cavities and in the extravasation of urine. extravasation of perirenal urine [4]. Removal cannot be be considered before 4-6 weeks. Treatment of the cause is the second essential stage of treatment. There however, there is no consensus on how to monitor the therapeutic efficacy and the onset of complications.
The rupture of the fornix is a mechanism for releasing the the hyperpressure exerted on the renal parenchyma, the renal sinus and the fascia of Gerota. Rupture during acute is of mechanical origin. In chronic pathologies, it is the progressive appearance of hydronephrosis linked to the reflux of associated with the reflux of urine into the pyelocecal tract which has an irritant effect on the urothelial tissue and responsible for an inflammatory reaction and fibrosis fibrosis [1,2]. Retroperitoneal fibrosis associated with mechanical compression of the lower ureter by the ovarian mass explains ureteral dilatation, the ultimate stage of which is rupture of the cavities. is rupture of the cavities.
The clinical signs are not specific, and renal colic is the most frequent, the diagnosis is most often delayed [3] In previous studies, fever and leukocytosis are most often absent, as in our case [4].
In addition to treating the cause, the treatment is based on antibiotic therapy to prevent infection of the urinoma, [5] and to insert a ureteral catheter percutaneous nephrostomy in the most severe cases. The literature acknowledges the performance of the double J catheter as first-line treatment in the treatment of fornix ruptures. By allowing emptying of the urinary tract, there is a reduction in pressure in the pyelo-caliceal cavities and in the extravasation of urine. extravasation of perirenal urine [4]. Removal cannot be be considered before 4-6 weeks. Treatment of the cause is the second essential stage of treatment. There however, there is no consensus on how to monitorthe therapeutic efficacy and the onset of complications.
Fornix rupture is an uncommon urological complication, frequently associated with lithiasic obstruction and less commonly with a tumor etiology. URO-CT plays a crucial role in confirming the diagnosis. The treatment involves initial urine diversion followed by addressing the underlying pathology.
None.
[1] Breun H., Csapo Z. and Sigel A. (1989). Fornix rupture--a review of pathophysiology and clinical aspects. Der Urologe Ausg A, 28: 329-333.
[2] Ferri E., Casoni G. L. C., Gemma M., Lidia D. A. and Laura M., et al. (2006). Rupture of the renal pelvis complicating a renal colic: Report of a case. Am J Emerg Med, 24: 383-385.
[3] Paajanen H., Kettunen J., Tainio, H. and Jauhiainen K. (1993). Spontaneous peripelvic extravasation of urine as a cause of acute abdomen. Scand J Urol Nephrol, 27: 333-336.
Google Scholar, Crossref, Indexed at
[4] Doehn C., Fiola L., Peter M. and Jocham D. (2010). Outcome analysis of fornix ruptures in 162 consecutive patients. J Endourol, 24: 1869-1873.
Google Scholar, Crossref, Indexed at
[5] Paajanen H., Kettunen J., Tainio, H. and Jauhiainen K. (1993). Spontaneous peripelvic extravasation of urine as a cause of acute abdomen. Scand J Urol Nephrol, 27: 333-336.
Google Scholar, Crossref, Indexed at
 Awards Nomination
Awards Nomination