PHONE
+44-7482-878921
+44-7482-878921
2376-0249
Clinical-Medical Image - International Journal of Clinical & Medical Images (2020) Volume 7, Issue 10

Author(s): Amine Jemel, Tarek Sendi, Mouna Bousnina, Khedija Soumer, Chaker Jaber and Adel Mrad*
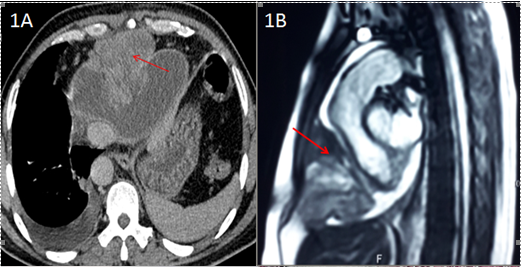
A 32-year-old man, with no pathological history, admitted to the cardiology department for a pronounced dyspnea. Computed tomography (Figure 1A) and thoracic magnetic resonance imaging (Figure 1B) revealed an anterior and lower mediastinal mass invading the pericardium with an intra-pericardial component compressing the right cavities without myocardial extension. The patient was operated on via a median sternotomy and the tumor has been completely removed (Figure 2A). Histopathological examination and immunohistochemical profile were compatible with a high grade undifferentiated myxoid sarcoma (Figure 2B). The post-operative was simple and the patient was referred to oncology for adjuvant chemotherapy. Primary malignant heart tumors are rare and pericardial neoplasms are even more exceptional. Among them, sarcomas are the most frequent histological type. Until now, there is no unequivocal clinical evidence guiding the management of pericardial sarcomas. Thus, a complete surgical resection is considered to be the cornerstone of therapy. Unfortunately, definitive surgical treatment is often not offered mainly due to the unresecability or associated comorbidities. Adjuvant chemotherapy and radiotherapy are not well defined. Therefore, primary pericardial sarcoma patients have poor prognosis.
 Awards Nomination
Awards Nomination