PHONE
+44-7482-878921
+44-7482-878921
2376-0249
Clinical Image - International Journal of Clinical & Medical Images (2021) Volume 8, Issue 10

Author(s): Hind Sahli*, Sanae Amalik, Jihane El Mandour, Hounayda Jerguigue, Rachida Latib and Youssef Omor
Commentary
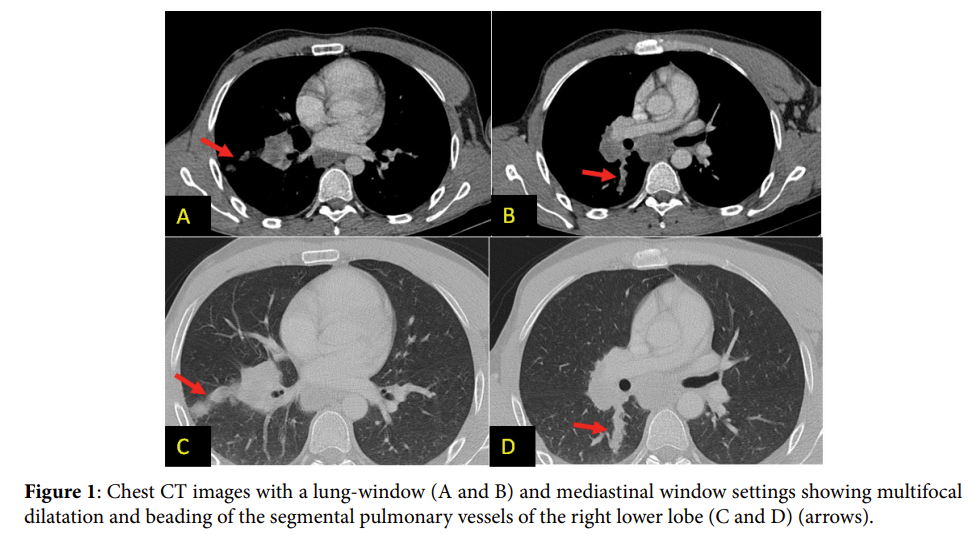
Pulmonary Tumour Embolism (TE) is a rare event. Neoplasms which are recognized to embolize the pulmonary arterial system include choriocarcinomas, renal cell, hepatocellular, and breast and stomach carcinoma [1]. We report a rare case of tumour embolism secondary to Ewing’s sarcoma that was investigated using chest CT scan. A 34-year-old man, followed up for pelvic extra-skeletal Ewing’s sarcoma, who is undergoing treatment with radio-chemotherapy. The patient presented left clavicle pain that gradually increased. No recent trauma had occurred. At the same time, the patient had been complaining for a few weeks of progressive dyspnea. Technetium-99 hydroxymethylene phosphate bone scans showed an increased uptake of the radioisotope at the middle of left clavicle. Computed Tomography (CT) showed sub periosteal localization of the lesion, the intact endosteal surface of the cortex, the absence of the soft tissue extension, and absence of matrix ossification and calcifications. CT scan showed also multifocal dilatation and beading of the peripheral sub segmental arteries of the right lower lobe, there was no peripheral wedge-shaped areas of attenuation due to infarction (Figure 1). Tumor embolism is a specific type of pulmonary embolism where the embolus includes either microscopic or macroscopic tumor components. It also represents an underestimated source of pulmonary embolism in sarcoma. It was first documented in 1897 by Schmidt, and most information on tumour emboli have been obtained from autopsy series or case reports [2-4]. Individuals with TE have a range of clinical findings from asymptomatic and chronic cor pulmonale to hemodynamic instability resulting in death [2]. TE in sarcomas usually presents acutely, whereas TE in non-sarcomatous settings is mainly subacute. Laboratory values are often revealing hypoxemia (usually Pao, <50mm Hg) and respiratory alkalosis [3]. The diagnosis is often unrecognized and mistaken with thromboembolism [1]. Anticoagulation and thrombolysis are not useful for TE and considered an absolute contraindication as it may result in haemoptysis [2]. Antemortem diagnosis is challenging and may not be established until post-mortem evaluation. In the early phase, most imaging studies are insensitive for making a diagnosis [4]. CT scan or CT angiography is considered the gold standard for the diagnosis of TE [2]. The scans revealed beaded appearance of the pulmonary vasculature, primarily in a subsegmental distribution involving multiple lobes [3]. In some cases, it is accompanied by tumour extension into the perivascular interstitium . Pulmonary infarction can be seen as a wedge-shaped pleural consolidation or a ground glass opacity with the apex directed towards the pulmonary hilum [5]. Other diagnostic modalities have also been suggested including ventilation perfusion scan, bone scintigraphy, angiogram, echocardiogram, and histologic verification using endoscopic bronchial ultrasound and pulmonary artery catheter aspiration. In our case, the diagnosis had been made with bone scintigraphy and CT scan. The treatment usually targets the primary malignancy [5]. Pulmonary tumour embolus is typically an end-stage manifestation of malignancy, and the prognosis with or without therapy is generally poor after onset of symptoms.
Declaration of Interests
The authors declare that they have no competing interests.
References
 Awards Nomination
Awards Nomination