PHONE
+44-7482-878921
+44-7482-878921
2376-0249
Clinical-Medical Image - International Journal of Clinical & Medical Images (2019) Volume 6, Issue 7

Author(s): Mustafa Ozgur Cirik, Oral Mentes, Meric Unver, Ali Alagoz and Sema Avci*
Introduction:
Acute eosinophilic pneumonia is an uncommon serious and rapidly progressive lung disease and it can cause mortal respiratory failure. The cause of this acute respiratory distress syndrome are smoking, medications, infections, inhalational exposures to drugs or dusts and idiopathic. Airway epithelial injury, endothelial injury, releasing of interleukin-33, eosinophilic infiltration, degranulation and lung inflammation are mechanisms of this acute respiratory syndrome. Acute eosinophilic pneumonia is diagnosed with following combination of clinical and radiological findings; fever of less than five days′ duration, hypoxemia, diffuse alveolar-interstitial opacities on chest graphy, bronchoalveolar lavage fluid consisting of >25% eosinophils, rapid response to corticosteroids and absence of parasitic, fungal, or other infections. Herein, we aimed to present a clinical image of 21-year-old male patient diagnosed with acute eosinophilic pneumonia due to cocaine inhalation.
Acute eosinophilic pneumonia is an uncommon serious and rapidly progressive lung disease and it can cause mortal respiratory failure. The cause of this acute respiratory distress syndrome are smoking, medications, infections, inhalational exposures to drugs or dusts and idiopathic. Airway epithelial injury, endothelial injury, releasing of interleukin-33, eosinophilic infiltration, degranulation and lung inflammation are mechanisms of this acute respiratory syndrome. Acute eosinophilic pneumonia is diagnosed with following combination of clinical and radiological findings; fever of less than five days′ duration, hypoxemia, diffuse alveolar-interstitial opacities on chest graphy, bronchoalveolar lavage fluid consisting of >25% eosinophils, rapid response to corticosteroids and absence of parasitic, fungal, or other infections. Herein, we aimed to present a clinical image of 21-year-old male patient diagnosed with acute eosinophilic pneumonia due to cocaine inhalation.
Case:
A 21-year-old male patient admitted to emergency room with complaints of progressive dyspnea, cough, sputum and hemoptysis. The patient did not have chronic disease or medical drug history. He has been smoking for five years. It was learned that he inhaled cocaine about 48 hours ago before the admission. On physical examination, bilateral decreased respiratory sounds, sibilant bronchus and bilateral basal roller were revealed. The vital signs of patients were following; tension arterial 110/70 mmHg, fever 38.1ºC, respiratory rate 31 per minute, heart rate 115 per minute and oxygen saturation on room air 65%. The arterial blood gas analysis was; pH 7.38, pO2 30 mmHg, pCO2 42 mmHg and SpO2 62. The complete blood count analysis was; white blood cell 22.16 (1000µL), eosinophil blood (%) 1.21 (normal range 0-0.7) and neutrophil count 18.6 (1000µL). The other blood parameters were normal. The culture in throat swab specimens was negative.
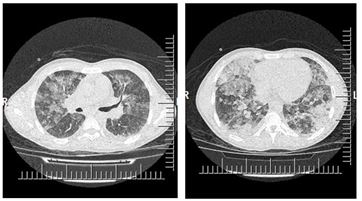
Chest computed tomography of the patient demonstrated diffuse ground glass opacities and minimal pleural fluid in the right hemithorax (Figure 1). The patient was hospitalized to the intensive care unit. On fiberoptic bronchoscopy, the mucosa was hyperemic, edematous and fragile. The cell counts from broncoalveolar lavage revealed more than 25% eosinophils. The clinical diagnosis of the patient was acute eosinophilic pneumonia and intravenous 2 mg/kg/day corticosteroid treatment was started. On the 10th day, complete improvement was shown on chest tomography (Figure 2). The patient’s clinical findings started to regress and he was discharged on the 11th day.
 Awards Nomination
Awards Nomination